
NEET Biology Notes Breathing And Exchange Of Gases Respiration
Respiration may be defined as the process in which oxygen is taken inside the body from the environment for the oxidation of food to release energy and the carbon dioxide so produced during oxidation is expelled out of the body.
The process of oxidation of food is complex. It involves a series of complex biochemical reactions and the released energy is stored in the form of ATP molecules. However, for simplicity sake, the multistep reaction can be briefly expressed as follows:
Types Of Respiration: Based on the mode of gas exchange between the body cells and the surrounding air, there are mainly two types of respiration: direct and indirect respiration.
1. Direct Respiration
- There is a direct exchange of gases between the carbon dioxide of body cells and the oxygen of water, and there is no blood for the transport of gases.
- The exchange of gases occurs on the principle of diffusion.
- It is found in unicellular organisms such as aerobic bacteria and protists (for example., Amoeba) and metazoans such as sponges, coelenterates (for example., Hydra), flatworms, roundworms, and insects.
2. Indirect respiration
- There is no direct contact between the body cells and the surrounding air or water.
- The source of oxygen is called the respiratory medium.
- Indirect respiration is found in larger and more complex forms of animals.
- These organisms have some specialized organs such as gills (most crustaceans, mollusks, insect larvae, and all fishes and amphibians), lungs (snails, amphibians, and all reptiles, birds, and mammals).
- In this mode of respiration, the transportation of oxygen and carbon dioxide between the respiratory organs and the body cells is brought about by the blood of the circulatory system.
All physical and chemical reactions in which atmospheric air oxidizes food in the body cells resulting in the production of energy and liberation of CO2 are included in respiration. Based on the mode of nutrient oxidation, respiration is of the following types:
Read and Learn More NEET Biology Notes
1. Anaerobic Respiration
- It occurs when nutrients are oxidized without using O2 (also called fermentation).
- In yeast, glucose forms ethyl alcohol and CO2. In bacteria and muscles, glucose is converted into lactic acid.
- Endoparasites also respire anaerobically.
- Anaerobic respiration is a low energy-yielding process.
- In mature RBCs also, anaerobic respiration occurs due to the loss of mitochondria along with other cell organelles.
2. Aerobic respiration
- Cells utilize O2 for oxidizing nutrients.
- O2 is used either from atmospheric air or from water. It involves:
- External respiration (breathing or ventilation): It is the exchange of oxygen present in the surrounding gaseous or liquid medium and carbon dioxide in the blood through a liquid medium by diffusion across the body surface or respiratory surface. It is purely a physical process that depends upon the principle of diffusion and no energy is produced.
- Internal respiration: It is the exchange of oxygen present in blood and carbon dioxide in the body cells through tissue fluid at the cellular level. Internal respiration involves energy production and is a physicochemical process.
- Cellular respiration: It is the utilization of O2 by cells for energy product; and result-dependent release of CO2.
Respiratory Organs In Animals
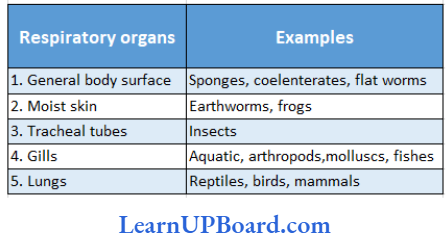
The process of exchange of O–, from the atmosphere with CO2 produced by the cells is called breathing, commonly known as respiration. Shows various examples of their specific respiratory organs.
” respiratory system notes “
Organisms With Their Specific Respiratory Organs:
NEET Biology Notes Breathing And Exchange Of Gases Human Respiratory System
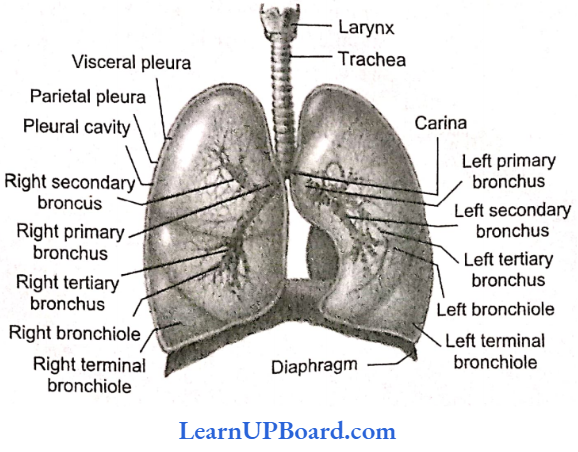
Shows the human respiratory’ pathway including the organs responsible for carrying out the gas exchange in the human body.
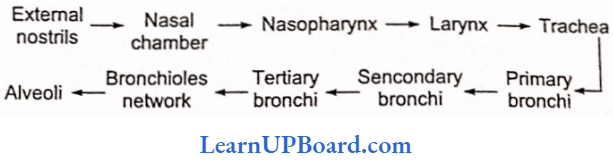
Following are the organs involved in carrying out the human respiration:
1. Nasal cavity
- The nasal cavity is the first part of the respirator)’ system.
- It opens to the exterior through the nostrils.
- The nasal cavity is divided into nasal chambers by nasal septum. Each nasal chamber can be differentiated into three regions:
- Vestibular region: The first part starting from the nostril has oil glands and hair to prevent the entry of large dust particles.
- Respiratory part: Highly vascular and involved in the conditioning of air as the air gets warmed and moist. Arising from the tire wall of each nasal chamber, there are three shallow’ bony ridges called nasal conchae. These are individually named as superior, middle, and inferior. Superior lies within the olfactory part; middle and inferior lie in the respiratory part. The conchae are covered with mucus membranes and greatly increase the surface of the nasal chambers.
Olfactory’part: It is the upper part, lined by olfactory epithelium for smell.
2. Pharynx
- From the nasal cavity, the air enters the pharynx.
- It serves as a common passage for both air and food.
- The opening into the windpipe or trachea is a narrow slit the glottis.
- The glottis is protected against the entrance of food by a triangular flap of tissue, the epiglottis.
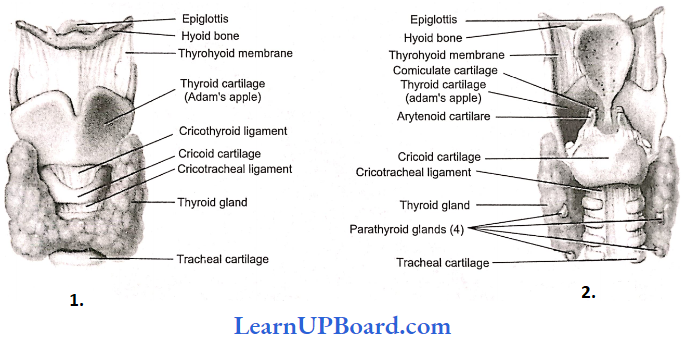
3. Human Larynx
- Until puberty, there is little difference in the size of the larynx (voice box) in males and females.
- The larynx opens into the tire oropharynx by a slit-like aperture, the glottis.
- The larynx is composed of irregularly shaped cartilages attached to each other by ligaments and membranes.
The main cartilages are:
- Thyroid cartilage: It is the most prominent, C-shaped, dorsally incomplete cartilage called Adam’s apple as it is apple-shaped and more prominent in males.
- Cricoid cartilage: It lies below the thyroid cartilage, and its shape is like a signet ring.
- Arytenoid cartilages: These are two roughly pyramid-shaped cartilages forming the posterior wall of the larynx. Corniculate cartilages: These are two conical nodules of elastic fibro-cartilage which lie at the apices of arytenoid cartilages.
- Cuneiform: These are two small, elongated, club-shaped nodules of elastic fibro-cartilage that lie above and anterior to corniculate cartilages. These connect epiglottis to arytenoid cartilage.
4. Trachea
- The trachea is a tube about 12 cm long with C-shaped (dorsally incomplete) rings of hyaline cartilage in its walls.
- These rings of cartilage make the wall non-collapsible.
- It is internally lined by pseudo-stratified ciliated columnar epithelium.
- Cilia beat to push out the mucus.
5. Bronchi
- The walls of the bronchi are likewise supported by cartilaginous rings.
- Each bronchus divides and redivides further into smaller bronchioles.
Epiglottis: It is a single leaf-shaped cartilage that projects into the pharynx.
- Thus, a total of nine cartilages are present, three paired (3, 4,5) and three unpaired (1,2, 4).
- The thyrohyoid membrane is a broad, flat membrane attached to the hyoid bone above and to the thyroid cartilage below.
- Inside the larynx are present two pairs of vocal cords, one pair of false vocal cords which have little to do with sound production, and the second inner pair of true vocal cords.
- When the air is forced through the larynx, it causes vibration of the true vocal cords, and sound is produced.
- The pitch of sound is determined by the tension on vocal cords. The greater the tension, the higher the pitch.
- Epithelium gradually changes from pseudo-stratified ciliated columnar epithelium in the bronchi to ciliated simple cuboidal epithelium in the terminal bronchiole.
- Incomplete rings of cartilage are gradually replaced by plates of cartilage that finally disappear in a distal bronchiole.
- The terminal bronchiole is further subdivided into respiratory bronchioles. Respiratory bronchioles open into alveolar ducts → atria → alveolar sacs → alveoli. From respiratory bronchioles onward, the wall is very thin and is made up of ol’ simple squamous epithelium.
gaseous exchange in humans
6. Lungs
- The lungs occupy the greater part of the thoracic cavity.
- Surrounding each lung is a double-walled sac within the walls of which lies the pleural cavity.
- The right lung is divided into three lobes and the left into two.
- Inside the lung, each bronchus divides into numerous bronchioles, each of which terminates into an elongated saccule, the alveolar duct, which bears on its surface air sacs or alveoli.
- The number of alveoli in the human lungs has been estimated to be approximately 300 million.
- The lungs are covered by a thin double layer of simple squamous epithelium called the pleura.
- The outer or parietal pleuron remains attached to the wall of the thoracic cavity.
- The space between the two pleural membranes contains pleural fluid for reducing friction and makes the movement of the lung easy.
- Inflammation of the pleura causes a disease called pleurisy.
- Lungs are pink at birth.
- They become dark grey and mottled in adults due to the deposition of carbonaceous materials.
- Darkening increases in smokers and persons exposed to pollutants.
- The right lung is shorter by about 2.5 cm due to the raised position of the diaphragm on the right side to accommodate the liver.
- The left lung is longer. It is, however, narrower than the right lung because it contains a cardiac notch for accommodating an asymmetrically placed heart. The left lung is divisible by an oblique fissure into two lobes, left superior and left inferior.
- The right lung has two fissures, horizontal and oblique. They divide the right lung into three lobes: right superior, right middle, and right inferior. The lobes are divided internally into segments and segments into lobules.
- There are eight segments in the left lung and 10 segments in the right lung. On average, an adult’s right lung weighs 625 g, while the left lung weighs 565 g.
NEET Biology Notes Breathing And Exchange Of Gases Mechanism Of Breathing
Respiratory movements in man are carried out with the help of intercostal muscles and diaphragm. There are two phases of each breathing movement, inspiration and expiration.
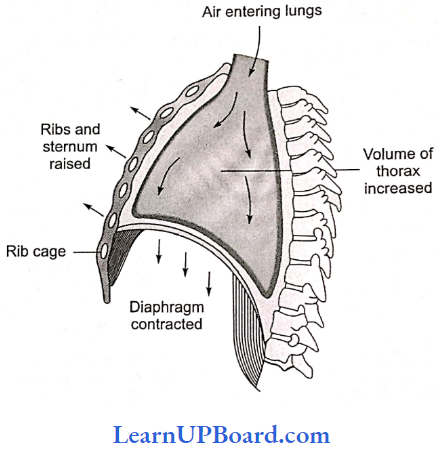
1. Inspiration (inhalation): It involves the intake of fresh air in the alveoli of the lungs. It includes an active process and consumes mechanical energy. There are two types of inspiratory muscles: phrenic and external intercostal muscles.
- Phrenic Muscles: These muscles extend from the diaphragm to the ribs and vertebral column.
- External Intervestal Muscles: These are 11 pairs of muscles present between 12 pairs of ribs dor- ventrally and laterally. When phrenic muscles contract, the diaphragm is flattened whereas when external intercostal muscles contract, the ribs are pulled forward, upward, and outward. The thoracic cavity increases in all directions which results in the increase in volume and decrease in pressure. So, air moves into the lungs.
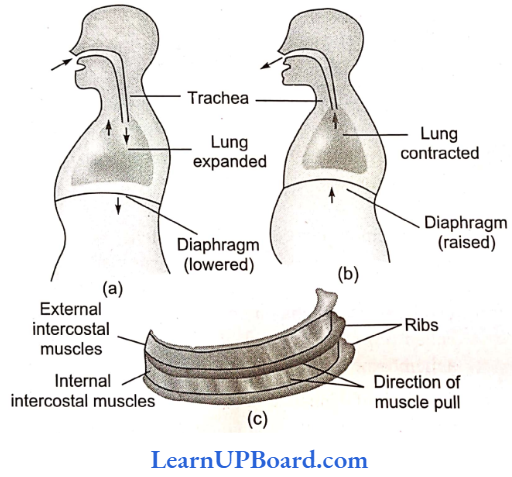
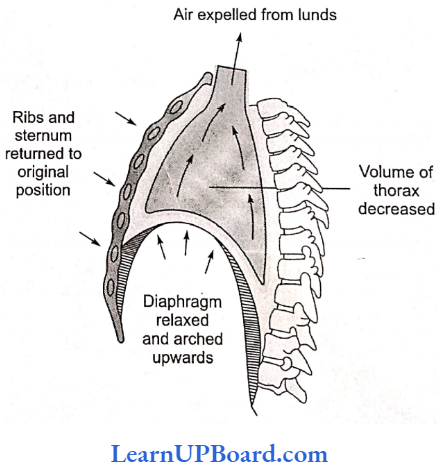
2. Expiration: It involves the expelling of air of high pco2 out of the body. During rest, the expiration is a passive process and simply involves the relaxation of inspiratory muscles (phrenic and external intercostal muscles). These decrease the volume of the thoracic cavity. But during forceful expiration, two expiratory muscles also help in expiration: the abdominal and internal intercostal muscles.
- Abdominal muscles: These extend front ribs to abdominal organs. When these muscles contract, the abdominal visceral organs are pulled upward, toward the diaphragm. So the diaphragm becomes more convex and the thoracic cavity decreases anteroposteriorly.
- Internal intercostal muscles: Like external intercostal muscles, internal intercostal muscles are also in 11 pairs present between the ribs. When these contract, ribs arc pulled backward, downward. and inward. So thoracic cavity decreases dorsoventrally and laterally. Due to the above changes, a larger amount of air is passed out.
Pulmonary Volumes
- Tidal volume (TV): It is the volume of air inspired or expired involuntarily in each normal breath. It is about 500 mL of air in an average young adult man.
- Inspiratory reserve volume (1RY): It is the maximum volume of air that a person can inhale over and above tidal volume by the deepest possible voluntary inspiration. It is about 2500 3000 mL.
- Expiratory reserve volume (ERV): It is the volume of air that can expire over and above the tidal volume with maximum effort. It is about 1000-1100 mL.
- Residual volume (RY): It is the volume of air left in the lungs even after maximum forceful expiration. It is about 1100— 1200
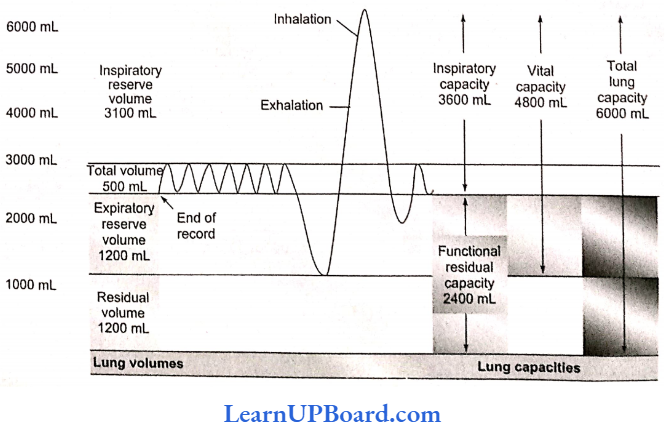
Pulmonary Capacities: Pulmonary capacities are the combination of two or more pulmonary volumes. These include
Inspiratory capacity (IC): This is equivalent to TV 4 IRV. It is about 3000-3500 rnL. Functional Residual Capacity (FRC): It is equivalent to ERV 4 RV. It is about 2500 mL. Vital capacity (VC): It is equivalent to IRV + TV + ERV. It varies from 3500 mL to 4500 mL depending on the age, sex, and height of a person.
Total lung capacity (TLC): It is equivalent to TV + IRV 4 RV + ERV. It is about 5800 mL. With the exception of FRC, RV, and TLC, all other lung values and lung capacities can be measured with the help of a simple spirometer. All pulmonary volumes and capacities are about 20-25% less in women than in men, more in athletic people than asthmatics.
Physiological Shunt And Shunted Blood: Whenever the ventilation/perfusion ratio is below normal, there is inadequate ventilation to provide the O2 required to fully oxygenate the blood flowing through the alveolar capillaries.
Therefore, a certain fraction of venous blood passing through the pulmonary capillaries does not become oxygenated. This fraction is called shunted blood. A small degree of shunt is nonthermal and may be described as a physiological shunt. Normally, this is about 2% of the cardiac output.
Physiologic Dead Space: When ventilation of some of the alveoli is great but alveolar blood flow (perfusion) is low, there is far more O2 available in alveoli than can be transported away from the alveoli by the flowing blood.
Hence, physiological dead space is the air that is inhaled by the body in breathing but does not take part in gaseous exchange. About one-third of every resting breath is dead space. In adults, it is usually in the range of 150 mL. Hence, shunt and dead space are due to deviations in the ventilation/perfusion ratio.
NEET Biology Notes Breathing And Exchange Of Gases Gaseous Exchange
- Alveoli are the primary sites of exchange of gases.
- The exchange of gases also occurs between blood and tissues.
- O2 and CO2 arc are exchanged in these sites by simple diffusion mainly based on pressure/concentration gradient.
- The solubility of gases as well as the thickness of membranes involved in diffusion are also among the important factors that can affect the rate of diffusion.
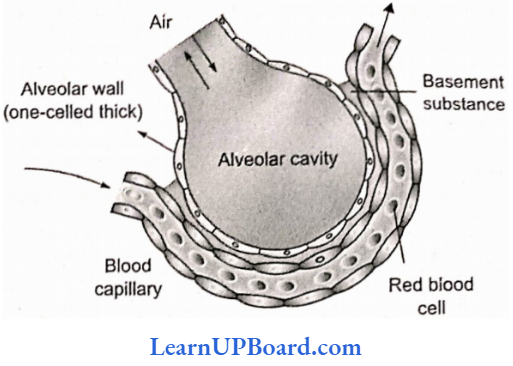
- The partition between the two includes alveolar epithelium, alveolar epithelial basement membrane, thin interstitial space, capillary basement membrane, and capillary endothelial membrane. This whole part is called the respiratory membrane and cumulatively forms a membrane of 0.5 μm thickness.
- The limit of exchange between alveoli and pulmonary blood is called diffusing capacity. It is defined as the volume of gas that diffuses through the respiratory membrane in one minute for a particle pressure difference of 1 mm Hg.
- Solubility of the gases in lipids also affects diffusing capacity.
- The diffusing capacity of CO2 is 20 times more than that of oxygen which is about double than that of nitrogen.
- Surfactant: A surface active agent lecithin secreted by type II alveolar epithelial cells reduces surface tension between the alveolar fluid and air. It prevents the collapsing of lung alveoli.
- The exchange of gases between the alveoli and blood in the lungs, and the blood and tissues is the result of differences in the partial pressure of respiratory gases, that is, oxygen and carbon dioxide.
External Respiration or Gaseous Exchange at Alveoli Level: The partial pressure of O2 in atmospheric air is 159 mm of Hg and that of CO2 is 0.3 mm of Hg.
- The partial pressure of oxygen po2 in alveolar air is 104 mm Hg and it is only 40 mm Hg in the arterial capillaries of lungs. Therefore, oxygen from the alveolar air rapidly diffuses into the blood capillaries due to its higher po2.
- In the expired air, it changes to 116 mm of Hg.
- Similarly, pco2 in the blood reaching the alveolar capillaries is 45 mm Hg whereas pco2 in the alveolar air is 40 mm Hg. Therefore, CO2 rapidly leaves blood capillaries and reaches alveoli.
- pco2 level in the expired air is 32 mm Hg.
Partial pressure (mm Hg) and percentage of respiratory gases during inspiration and expiration:
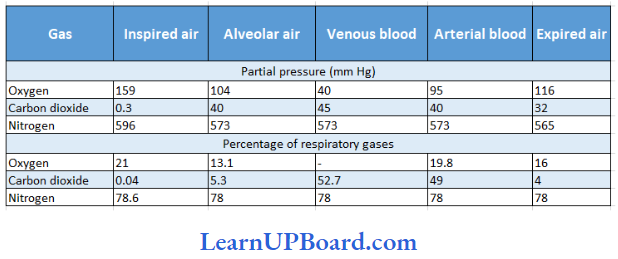
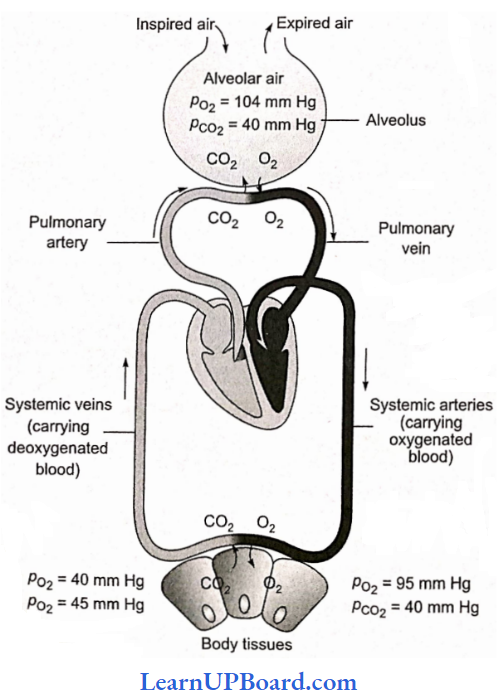
Internal Respiration or Gaseous Exchange at Tissues Level: The gaseous exchange between blood and body tissues is also due to differential partial pressures. The po2 and po2 of the arterial blood reaching the tissues are 95 and 40 mm Hg, respectively. The po2 and pco2 °f tissues are 20 and 52 mm Hg, respectively. Therefore, oxygen quickly leaves the blood and enters the cells whereas CO2 produced in the tissues leaves the cells and enters the blood.
NEET Biology Notes Breathing And Exchange Of Gases Factors That Decrease Oxygenation
Various factors responsible for the decrease in the combination of oxygen with blood are as follows:
- Low blood volume
- Anemia
- Low Hb
- Poor blood flow
- Pulmonary diseases
NEET Biology Notes Breathing And Exchange Of Gases Transport Of Gases In Blood
The exchange of oxygen and carbon dioxide takes place in between the lungs and blood. The greater part of oxygen diffuses into the blood, and at the same time, carbon dioxide diffuses out. Below are explained two types of gas transport systems: oxygen transport and carbon dioxide transport.
Oxygen Transport
- Each deciliter of blood carries 19.8 mL of O2 ol which 5 mL diffuses into tissues.
- 3% of O2 transported is dissolved in plasma and 97% is carried by RBCs. Four Fe2+ ions of each hemoglobin can bind with four molecules of O2 and it is carried as oxyhemoglobin.
Hb4+4O2 → HB4O8
- Oxyhemoglobin dissociates near tissues due to an increase in acidity and a decrease in pH. It can also be caused due to high temperatures.
- In a normal person, the hemoglobin level is about 15 per 100 mL.
- The capacity of 1 g of hemoglobin to combine with O2 is 1.34 mL. Therefore, arterial blood carries about 20 mL of O2/100 mL of blood.
- Under normal conditions, the O2 level falls to about 14.4 mL/100 mL in the venules.
- It indicates that under normal conditions, approximately 5 mL of oxygen is transported by blood.
- Under strenuous conditions or during exercise, the O2 level falls to about 4.4 mL/100 mL, i.e., approximately 15 mL of O2 is transported by Hb during exercise.
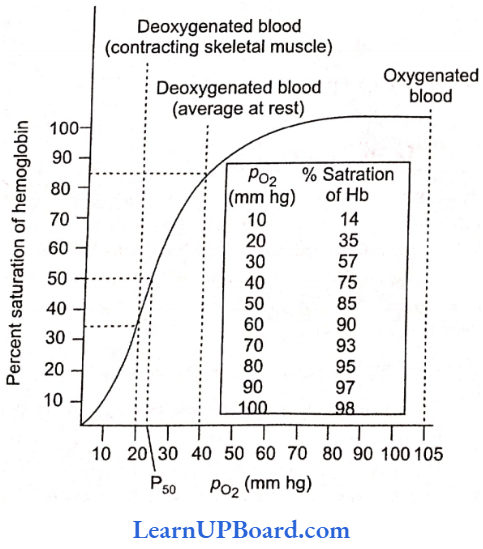
- Bohr’s effect: The relationship between po2 and the percent saturation of hemoglobin when represented on a graph is termed an oxygen-hemoglobin dissociation curve and is sigmoid in shape. A rise in pco2 or fad in pH decreases the oxygen affinity of hemoglobin, raising the p50 value. This is called Bohr’s effect (p50 value is the value of po2 at which hemoglobin is 50% saturated with oxygen to form oxyhemoglobin).
- Conversely, a fall in pco2 and a rise in pH increase the oxygen affinity of hemoglobin and shift the curve to the left. Fetal hemoglobin has a higher affinity for 02 because it binds BPG less strongly. Therefore, the oxygen-hemoglobin dissociation curve for fetal hemoglobin will appear on the left side.
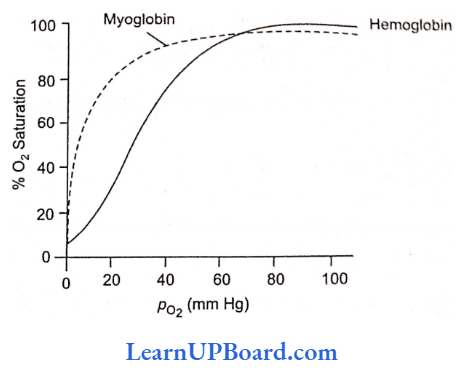
Myoglobin present in the muscles also has more affinity for O2. But since it has only one he’ group, the curve obtained will be hyperbolic, not sigmoid.
NEET Biology Notes Breathing And Exchange Of Gases Points To Remember
Carbon monoxide poisoning: If a person sleeps in a closed room with a lamp burning, the absence of a sufficient amount of oxygen causes an incomplete combustion of carbon and produces carbon monoxide in the room. As the person inhales carbon monoxide, it diffuses from the alveolar air to the blood and binds to hemoglobin forming carboxyhemoglobin. The latter is a relatively stable compound and cannot bind with oxygen.
” notes on respiratory system”
So, the amount of hemoglobin available for oxygen transport is reduced. The resulting deficiency of oxygen causes headaches, dizziness, nausea, and even death. Carbon monoxide combines with hemoglobin at the same point on the hemoglobin molecule as oxygen. It binds with hemoglobin 250 times faster than oxygen.
SARS (severe acute respiratory syndrome)
- The first patient of SARS was reported on February 26, 2003, in China.
- The causative agent is human coronavirus.
- It is a new member of the influenza virus family which is considered a mutant form of the influenza virus.
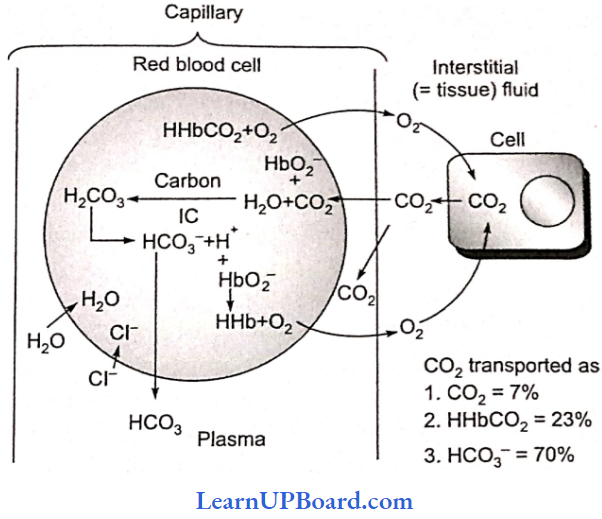
Carbon Dioxide Transport
CO2 is transported in three ways:
1. In dissolved state: About 7% of CO2 is transported after getting dissolved in plasma. The pco> in arterial blood is 40 mm of Hg and in venous blood, it is 45 mm of Hg. About 0.3 mL of extra CO: is carried per 100 mL of blood in this form.
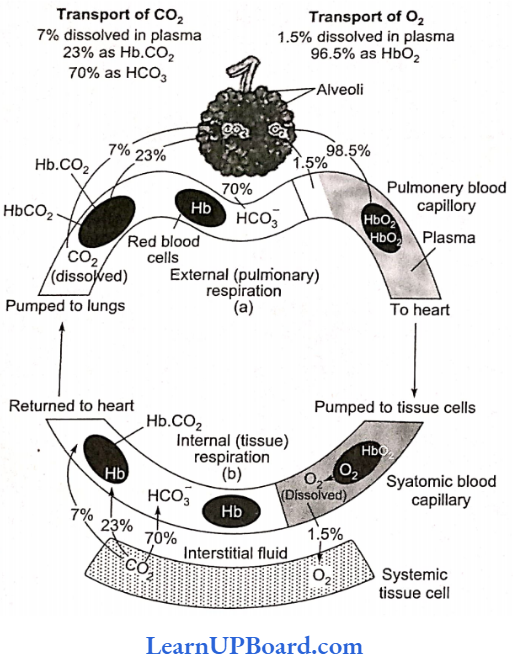
2. As bicarbonate: Nearly 70% of CO2 is transported from tissues to lungs in this form. CO2 diffuses from tissues into the blood and enters RBCs. It combines with water to form H2CO3 which dissociates into H+ and HCO3T Being catalyzed by carbonic anhydrase, it is a fast step.

H+ ions combine with hemoglobin replacing its association with K+ and forming hemoglobinic acid.
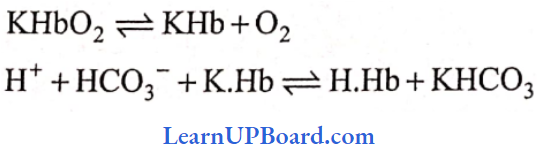
Due to this, the level of HCO3– increases in RBCs, which start coming out of it along the concentration gradient. To maintain ionic balance, Cl– moves in from plasma into RBCs. In the plasma, HCO3– combines with Na+ or K+ to form NaHCO3 or KHCO3.
3. As carbamino-Hb: About 20-25% of CO2 is transported in this mode. CO2 combines with the NH2 group of Hb and forms carbamino-Hb. This combination of CO2 and Hb is a reversible reaction.
Release of CO2 in the alveoli of the lung: In the pulmonary capillaries, CO2 starts diffusing out into the alveoli.
- Carbamino-Hb spits into CO2 and Hb. As Hb of RBC takes up O2, it releases H+ in RBC.
- H+ starts combining with the available HCO3– in RBC to form H2CO3 which splits into H2O and CO2, and CO2 starts diffusing out (reverse of reactions).
- As a result, HCO3– from plasma starts moving in along the concentration gradient, and for ionic balance, Cl-starts move out. This way CO2 is released into the lungs.
Hamburger’s phenomenon: HCO3 ions diffuse out into plasma and Cl– ions enter into the RBCs at the level of tissues (internal respiration). This is known as the chloride shift or Hamburgers phenomenon. At the level of external respiration or alveoli, Cl– moves out as HCO3– moves in. This is called the reverse of the chloride shift.
Haldane’S Effect
- It is related to the transport of CO2 in the blood. It is based on the simple fact that oxyhemoglobin behaves as a strong acid and releases an excess of H+ ions which bind with bicarbonate (HCO3–) ions to form H2CO3 which dissociates into H2O and CO2.
- Secondly, due to increased acidity, CO2 loses the power to combine with hemoglobin and form carbamino-hemoglobin.
- The effect of oxyhemoglobin formation or dissociation on CO–, transport is called Haldane’s effect.
NEET Biology Notes Breathing And Exchange Of Gases Regulation Of Breathing
1. Respiratory Center
- As the breathing muscles are voluntary, the breathing pattern can be altered voluntarily (cerebral cortex activity).
- The normal respiratory rhythm (12-14 min) is controlled by the nervous system (mainly the medulla).
- Three groups of respiratory centers are involved—dorsal respiratory group, ventral respiratory group, and pneumotaxic center.
- The signals from the dorsal respiratory group (located in the dorsal portion of the medulla) are transmitted to the diaphragm and maintain normal breathing patterns.
- The ventral respiratory group (located anterolaterally to the dorsal inspiratory group) is involved only in enhanced respiratory requirements. It regulates both inspiration as well as expiration.
- The pneumatic center is located in the pons and controls the switch-off point of inspiration.
- When sending a weak signal, inspiration lasts for about 5 seconds causing complete filling of the lungs.
- When sending a strong signal, the rate of breathing increases, i.e., the duration of inspiration and expiration decreases and complete filling of lungs is not possible.
2. Chemical control
- Central chemoreceptors are present in the medulla oblongata (CNS) whereas the peripheral chemoreceptors are located in the walls of systemic arteries (aortic body with aortic arch and carotid body with carotid artery).
- They relay impulses to the respiratory center over the cranial nerves of PNS.
- Increased pco2, increased H+ concentration, and decreased po2 input from the central and peripheral chemoreceptors cause the inspiratory area to become highly active, and the rate and depth of breathing increase.
- Severe hypoxia depresses the activity of central chemoreceptors and the respiratory center.
- The respiration rate decreases or breathing ceases altogether, and po2 falls lower and lower (asphyxia).
NEET Biology Notes Breathing And Exchange Of Gases Disorders Of The Respiratory System
Asthma: It is difficulty in breathing, causing wheezing due to inflammation of the bronchi and bronchioles.
Emphysema: It is a chronic disorder in which alveolar walls are damaged due to which the respiratory surface is decreased. One of the major causes of this is cigarette smoking.
Occupational respiratory disorders: In certain industries, especially those involving grinding or stone-breaking, so much dust is produced that the defense mechanism of the body cannot fully cope with the situation. Long exposure can give rise to inflammation leading to fibrosis (proliferation of fibrous tissues) and thus causing serious lung damage. Workers in such industries should wear protective masks.
Bronchitis: It is the inflammation of the bronchi which is characterized by hypertrophy and hyperplasia of scro-mucous glands and goblet cells lining the bronchi. The symptom is regular coughing with thick greenish-yellow sputum that indicates the underlying infection, resulting in the excessive secretion of mucus. It may also be caused by cigarette smoking and exposure to air pollutants like carbon monoxide.
” gas exchange in humans”
Bronchial asthma: This is characterized by spasms of the smooth muscles present in the bronchiole walls. It is generally caused due to hypersensitivity of the bronchiole to foreign substances present in the air passing through it. The symptoms of the disease may be coughing or difficulty in breathing mainly during expiration. The mucus membranes on the wall of the air passage start secreting excess amounts of mucus, which may clog the bronchi, as well as bronchioles.
Pneumonia: It is the infection of the lungs by Streptococcus pneumoniae and leads to the accumulation of mucus and lymph containing dead WBCs in alveoli, impairing gaseous exchange. Uptake of oxygen is adversely affected, and as a result, the oxygen level of the blood falls. Sometimes, it may be caused by other bacteria or fungi, protozoans, viruses, and mycoplasma.
Occupational lung disease: It is caused because of exposure to potentially harmful substances such as gas, fumes, or dust present in the environment where a person works. Silicosis and asbestosis are common examples, which occur due to chronic exposure of silica and asbestos dust in the mining industry. It is characterized by the fibrosis (proliferation of fibrous connective tissue) of the upper part of the lung causing inflammation.
Prevention and cure: Almost all occupational lung diseases express symptoms after chronic exposure, i.e., 10-15 years, or even more. Not only this, diseases such as silicosis and asbestosis are incurable. Hence, the person likely to be exposed to such irritants should adopt all possible preventive measures. These measures include:
- Minimizing the exposure of harmful dust at the workplace.
- Workers should be well-informed about the harm of the exposure to such dust.
- Use of protective gear and clothing by workers at the workplace.
- Regular health check-ups.
- Holiday from duty at short intervals for workers in such areas.
- The patient may be provided with symptomatic treatment such as bronchodilators and antibiotics in order to remove the underlying secondary infection.
Tuberculosis: A bacterial disease caused by Mycobacterium tuberculosis. This decreases the elasticity of the lungs making them fibrous.
Whooping cough or pertussis: An infectious disease caused by the bacterium Bordetella pertussis.
Sleep apnoea syndrome (SAS): Persons with snoring habits suffer from sleep apnoea syndrome because their respiratory tract closes on inhalation.
Cough: A reflex in lower respiratory passages followed by forceful expulsion of air to remove an irritant.
Sneeze: A reflex similar to cough but applies to nasal passageways instead of lower respiratory passages.
Hypercapnia: Excess of CO2 in the body.
Cyanosis: This means blueness of skin because of the excessive amount of deoxygenated Hb.
Periodic breathing: A breathing characterized by slowly waxing and waning respiration occurring over and over again about every 40-60 s. The acute effects of voluntary hyperventilation demonstrate the interaction of the chemical respiratory regulating mechanisms.
- When a normal individual hyperventilates for 2-3 min, then stops and permits respiration to continue without exerting any voluntary control over it, there is a period of apnea. This is followed by a few shallow breaths and then by another period of apnea, followed again by a few breaths (periodic breathing).
- The cycles may last for some time before normal breathing is resumed. The apnea apparently is due to CO2 lack because it does not occur following hyperventilation with gas mixtures containing 5% CO2. During an apnea, the alveolar Po2 falls and PCo2 rises.
- Breathing resumes because of hypoxic stimulation of the carotid and aortic chemoreceptors before the CO2 level has returned to normal.
- A few breaths eliminate the hypoxic stimulus and breathing stops until the alveolar Po, falls again. Gradually, however, Pco2 returns to normal, and normal breathing resumes. Periodic breathing occurs in various disease states and is often called Cheyne-Stokes respiration.
Atelectasis: It means the collapse of the alveoli. When a bronchus or bronchiole is obstructed, the gas in the alveoli beyond the obstruction is absorbed and the lung segment collapses. The collapse of the alveoli is called atelectasis.
- The atelectatic area may range in size from a small patch to a whole lung. Some blood is diverted from the collapsed area to better-ventilated portions of the lung and this reduces the magnitude of the decline in arterial Po2. When a large part of the lung is collapsed, there is an appreciable decrease in lung volume.
- The intrapleural pressure, therefore, becomes more negative and pulls the mediastinum, which in humans is a fairly flexible structure to the affected side. Another cause of atelectasis is the absence or inactivation of surfactant, the surface tension depressing agent normally found in the thin fluid lining the alveoli.
- This abnormality is a major cause of failure of the lungs to expand normally at birth. The collapse of the lung may also be due to the presence in the pleural space of air (pneumothorax), tissue fluids (hydrothorax, chylothorax), or blood (hemothorax).
NEET Biology Notes Breathing And Exchange Of Gases Points To Remember
Terms associated with breathing
- Eupnea: Nonnal breathing
- Hypopnea: Slow breathing
- Hyperpnea: Rapid breathing
- Apnea: No breathing
- Dyspnea: Painful breathing
- Orthopnea: Difficult breathing except in an upright position
- Tachypnea: Rapid shallow breathing
- Chronic obstructive pulmonary disease (COPD): Examples, are emphysema, and chronic bronchitis.
Artificial respiration
- Artificial respiration may be required whenever breathing is depressed or absent, for example. during drowning, cardiac arrest, electric shock, carbon monoxide poisoning, or a head injury.
- A variety of methods of artificial respiration can be used.
- The commonly used methods are mouth-to-mouth respiration, mouth-to-nose ventilation, resuscitator, tank respirator, etc.
- Mouth-to-mouth respiration: In this, the patient is placed on his back on a firm surface. The head is kept at a slightly lower level than his stomach.
- The mouth and throat are cleared off from the mucus, food, etc. The operator closes the patient’s nostrils to prevent the leakage of air, takes a deep breath, and blows into the patient’s mouth until the chest is seen to rise. The operator then takes his mouth quickly away to allow passive exhalation. The process is repeated about 10-15 times a minute in adults.
- A normal person can usually survive as much as 20 mm Hg of continuous positive pressure in the lungs, but exposure to more than 30 mm Hg for a few minutes may cause death.
NEET Biology Notes Breathing And Exchange Of Gases Assertion Reasoning Questions
In the following questions, an Assertion (A) is followed by a corresponding Reason (R). Mark the correct answer.
- If both Assertion and Reason are true and the Reason is the correct explanation of the Assertion.
- If both Assertion and Reason are true, but the Reason is not the correct explanation of the Assertion.
- If Assertion is true, but Reason is false.
- If both Assertion and Reason are false.
Question 1. Assertion: The pneumatic center controls the rate of respiration.
Reason: Primarily, it controls the switch-off point of inspiration.
Answer: 1. If both Assertion and Reason are true and the Reason is the correct explanation of the Assertion.
Question 2. Assertion: Asthmatic patients use bronchodilator drugs as well as inhalers for symptomatic relief.
Reason: Asthma is characterized by the spasm of smooth muscles in the wall of bronchioles due to allergen.
Answer: 1. If both Assertion and Reason are true and the Reason is the correct explanation of the Assertion.
Question 3. Assertion: A major part of carbon dioxide is transported in the form of sodium bicarbonate.
Reason: 0.3 ml of carbon dioxide is transported per 100 mL of blood in dissolved shite in the plasma of blood.
Answer: 2. If both Assertion and Reason are true, but the Reason is not the correct explanation of the Assertion.
Question 4. Assertion: In cockroaches, inspiration is a passive process.
Reason: The expansion of the abdominal cavity allows the space for expansion of the tracheal trunk. As a result, air enters through spiracles.
Answer: 1. If both Assertion and Reason are true and the Reason is the correct explanation of the Assertion.
Question 5. Assertion: The diffusion of carbon dioxide is 20 times faster than oxygen.
Reason: It is due to the difference in partial pressure as well as the solubility of diffusing gases.
Answer: 1. If both Assertion and Reason are true and the Reason is the correct explanation of the Assertion.
Question 6. Assertion: Oxidation of nutrients releases bond energy.
Reason: Oxidation of nutrients is done by using molecular oxygen.
Answer: 2. If both Assertion and Reason are true, but the Reason is not the correct explanation of the Assertion.
Question 7. Assertion: Aerobic respiration involves the exchange of respiratory gases twice.
Reason: Exchange occurs from lung to heart and then heart to lung.
Answer: 3. If Assertion is true, but Reason is false.
Question 8. Assertion: Respiratory gas exchange occurs through os mosis.
Reason: Respiratory gas goes from the lower partial pressure region to the region of higher partial pressure.
Answer: 4. If both Assertion and Reason are false.
Question 9. Assertion: The first step of gas exchange occurs through the body surface in some animals.
Reason: The body surface or membrane of amphibia is thick in nature.
Answer: 3. If Assertion is true, but Reason is false.
Question 10. Assertion: Abdominal muscle is related to respiration in animals.
Reason: Relaxation of abdominal muscles draws in air.
Answer: 1. If both Assertion and Reason are true and the Reason is the correct explanation of the Assertion.